INTRODUCTION
The incidence of shoulder injuries in handball worldwide is considerable, being among the most frequent traumas leading to long-term sports inactivity or even early termination of sports careers. The most recent report presented by the International Olympic Committee indicates an injury rate ranging from 8.9 to 42.3 injuries per 1000 match hours and between 1.8 and 3.7 per 1000 training hours [1, 2].
A gradually applied training based on well-established criteria is essential to ensure the smooth progress of the recovery procedure, and the application of kinetoprophylaxis programs combined with recovery programs but also with psychological support programs are the desiderata of a perfect recovery act. The application of the recovery protocol will always take into account the principle of gradual effort dosage, the presence of pain in the joint of interest, the degree of loading, the recovery periods after competitions and training, the existing body dyskinesias, because all together form an important pillar that if neglected will produce consistent imbalances during the recovery process [3, 4, 5].
Following these steps contributes to a healing in the shortest possible time, so that the junior handball player can return to training and subsequently to competition and reach the performance threshold prior to the moment of injury.
The topicality and complex study of the subject addressed resides both in the analysis of indicators regarding the very large number of injuries occurring at the shoulder level among junior handball players, which come with long-term sports inactivity or even giving up on a high-performance sports career. as well as in the substantial need to create and implement modern and complex recovery programs in accordance with the needs of the consumer society [6]. Taking into account the aforementioned aspects, the importance of the subject is also supported by the need to regulate and update all research studies conducted in the country, but also in the European context by replacing rudimentary recovery protocols with modern, more complex ones in terms of providing physiotherapy recovery of shoulder injuries in junior handball players, with the aim of increasing the quality of life of the athletes, decreasing the recovery time and restoring the injury while eliminating relapses as much as possible [7, 8].
The aim of this study was therefore to show how the presence of shoulder injuries in junior handball players can affect the quality of life of young athletes and how we can eliminate the predisposing factors for the occurrence of injuries in young handball players. Junior handball players between the ages of 14 and 18 included in the study were evaluated during three competitive seasons, were monitored daily regarding recovery activity, the amount of effort put into training, but also during competitions. The primary goal is to analyze the degree of performance regarding the quality of life of these athletes and other problems that arise with it, but also how these dysfunctions disrupt sports activity but also everyday life [9].The results of the study highlight how the frequent occurrence of shoulder injuries in junior handball players leads to long-term inactivity, decreased sports performance and thus, the need to implement recovery and rehabilitation programs to recover from these injuries with improved parameters regarding quality of life [10, 11].
Playing competitive handball, especially at a junior age, comes with a number of disadvantages, including repeated injuries, which when not treated seriously lead to long-term sports inactivity accompanied by pain, irritability and an unsatisfactory quality of life due to a depressive emotional state that most often accompanies the injury.
A large study conducted within the Concussion Assessment, Research, and Education Consortium aimed to highlight the relationship between emotional state and sports traumatology and how repeated exposure to overtraining, failure to comply with prophylactic and recovery protocols, is followed by serious injuries that produce imbalances in the mental, physical and cognitive health of handball athletes and beyond. The results highlight how sports traumatology impacts the quality of life of athletes both in the short term and in the long term, where we are talking about an injury that can lead to the end of a sports career. Reports on the number of injuries in handball highlight an increasing trend and most often, against the background of injuries, there is also a depressive state and a decrease in the quality of life of athletes even many years after the injury, suggesting a correlation between the high number of injuries - depression - low quality of life score [12,13].
Participants in high-contact sports have a 5-fold higher risk of sustaining an injury during a competitive season compared to participants in other sports, and therefore psychological support from teammates seems to be a reliable ally that significantly contributes to reducing recovery time and improving the quality of life score. It seems that there is a direct relationship between emotional comfort, quality of life and the duration of practicing competitive sports, which contributes to the athlete's psychological resilience and emotional adaptation. However, the number of injuries, their severity and emotional health are important factors in determining the quality of life score [14]. In this regard, we identified some factors that have the role of influencing the quality of life score (image 1).
Image 1. Factors that influence the quality of life score
Junior handball athletes with more than one injury during a competitive season had significantly lower quality of life scores than athletes who experienced a single injury episode, also indicating a poor emotional state due to episodes of pain, irritability, and limited activities in daily life, but practicing team sports can be a compensating factor and can be seen as a benefit in the economy of the recovery act.
During handball training, emphasis will be placed on a sufficient warm-up period, on developing teamwork capacity, and taking into account the principle of gradualness and dosage of effort with alternating rhythm, duration, and difficulty. Protecting the overused joint in handball, namely the shoulder, by introducing prophylactic and strengthening programs is the key to success in limiting the occurrence of injuries and recording the best possible score in terms of quality of life [15,16,17].
At the same time, ensuring coherence between the principles applied in handball training and modern directions of sports education, which support an integrated approach to physical training and at the same time focus on prevention, performance and well-being [18,19]. Thus, the emphasis placed in handball on adequate warm-up, development of teamwork capacity and compliance with the principle of gradualness and dosage of effort correlates with the need to monitor motor parameters, well-being and the use of modern technologies to optimize the training process [20]. The introduction of prophylactic and strengthening programs to protect the shoulder joint reflects, in this context, the constant concern for maintaining the health of athletes, for increasing the quality of life and social integration through physical activity [21].
In addition, the integration of periodic functional assessments and individualized feedback into the training process contributes to the efficient adaptation of effort tasks, increasing athletes' motivation and strengthening preventive behavior oriented towards the longevity of sports practice and maintaining an optimal level of quality of life [22, 23, 24].
MATERIAL AND METHODS
The presented experiment lasted from September 2022 to July 2023 and 50 junior handball athletes were included in the study. The investigation was carried out in several directions, assessing the limitation of activities and the degree of dysfunction of the junior handball athletes included in the study, but also how the quality of life of the handball athletes present in the study is affected.
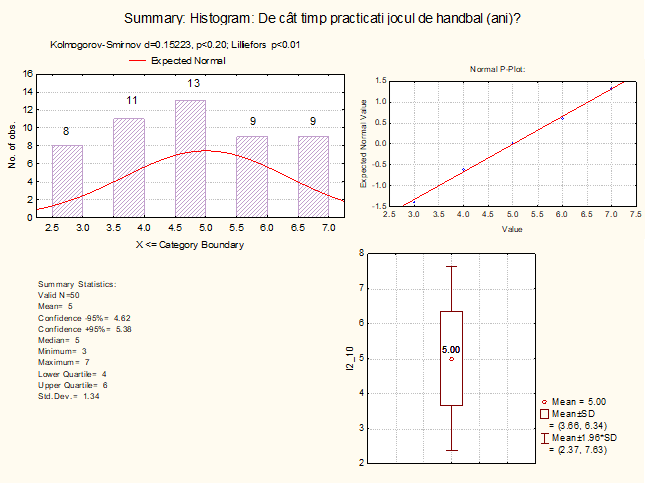
The group of junior handball players included in the study was homogeneous in terms of age with a mean age of (17.32±1.09SD) and did not present statistically significant differences and the duration of handball practice has an average value of 5 years with a standard deviation of 1.34, with minimum values of 3 years and maximum values of 7 years.
For a clearer analysis of the degree of disability and the level of functional impotence installed at the level of the shoulder joint, we developed and applied a questionnaire to highlight the limitation of activities. The questionnaire is based on 8 items that made it appropriate to analyze the performance of professional, sports and daily activities in order to conclude the degree of impairment and implicitly the level of impairment regarding the quality of life score of the athletes involved in the program.
The analysis and interpretation of the data from this questionnaire indicates that a significant number of handball players face a very high degree of disability due to the limitation of activities at the shoulder level, pain being the most common symptom among the players, respectively at 47.5% of the participants, while 48% experience a blockage caused by pain when it is necessary to raise the arm above the head, both with load and in free mode. In addition, 58% of the participants in this study state that they face multiple episodes of insomnia due to the pain installed at the joint level where the lesion is located.
We summarize that the level of limitation in the traumatized joint is significant,
and produces severe imbalances within the training and competition program and a well-developed kinetic program that masterfully combines physiotherapy techniques and means with technical exercises from handball practice is urgently necessary in order to be able to bring a correction to the coefficient that analyzes the quality of life of the athletes but also to return to the handball team training in the shortest possible time, without the risk of re-injury, because the return will be made when the shoulder joint is completely restored and consolidated.
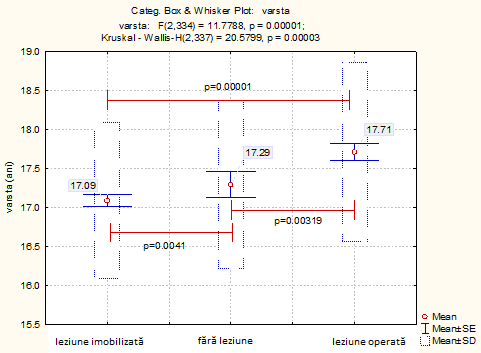
Following the analysis of the values obtained in this study, the target group where the incidence is highest is highlighted, namely juniors aged 15 - 18, score values regarding the degree of limitation in the range 11 - 17, with a general average of 15.13 ± 2.87 as can be seen in Table 2.
The results of the group of handball athletes highlight a very large number of athletes who register low values of the score regarding the limitation of activities within the joint under research, with a value of p> 0.05, which demonstrates the presence of homogeneity in the analyzed group.
| Lot | Average Score | Confidence interval | Dev.std | Min | Max | Q25 | Mediana | Q75 | |
|---|---|---|---|---|---|---|---|---|---|
| Lot | Average Score | -95% | -95% | Dev.std | Min | Max | Q25 | Mediana | Q75 |
| Handball players | 15.13 | 13.04 | 15.24 | 2.87 | 7.00 | 23.00 | 11.00 | 13.50 | 16.00 |
| Test statistic: ANOVA, F(1, 48) =0.1592, p=0.6916 Levene Test of Homogeneity of Variances: F=1.1754, p=0.2837 | |||||||||
The assessment of the score regarding the limitation of activities at the level of the injured shoulder revealed low values in both the analyzed group (14.14±3.87) with a minimum of 7.00 and a maximum value of 23 for the analyzed junior handball players. The analysis of the obtained values clearly indicates the existence of disability at the level of the injured shoulder and is accompanied by pain and irritability, with disturbances of rest/sleep periods and difficulties in performing daily tasks of activities, at the level of the injured shoulder in both analyzed groups. There were no significant differences between the junior handball players (P = 0.6917) in terms of the score regarding the limitation of activities at the level of the studied shoulder.
The evaluation of upper limb dysfunction was based on the application of the DASH questionnaire, which clearly highlights a high rate of cases recording values in the range of 65-75 regarding the dysfunction of the limb involved in the case study. As can be seen in Table 3, the group of female athletes participating in the study recorded DASH score results indicating significant shoulder dysfunction, from moderate to severe, but the group was homogeneous and normal.
| Lot: | Average DASH | Confidence Interval | Dev std | Min | Max | Q25 | Med. | Q75 | |
|---|---|---|---|---|---|---|---|---|---|
| Lot: | Average DASH | -95% | -95% | Dev std | Min | Max | Q25 | Med. | Q75 |
| Handball players | 59.67 | 56.22 | 63.12 | 12.15 | 32.54 | 92.73 | 51.31 | 58.38 | 66.31 |
| Test statistic: ANOVA, F(1, 49) = 1.4673, p=0.2421 Levene Test of Homogeneity of Variances: F=1.8251, p=0.0821 | |||||||||
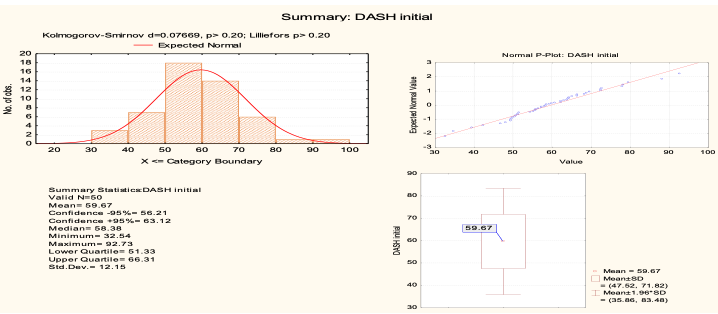
The mean DASH values did not show significant differences (P = 0.2329) between the
analyzed junior handball players, with a mean value of 59.67 ± 12.15, recording a minimum value of 32.54 and a maximum value of 92.73.
Regarding the assessment of the quality of life in the experimental group (©2003 Burckhardt and Anderson), the results of the quality of life questionnaire highlighted the fact that the analyzed athletes are a homogeneous group from the perspective of quality of life, so there were no significant differences in the qualitative analysis of the score (P = 0.2636) (Table 3, Table 4).
| Score | Interpretation | Lot of junior handball players n (%) |
|---|---|---|
| 1 – 40 | Dysfunctional perception of one's own life. | 8 (24%) |
| 40 – 70 | Serious perception | 24 (40%) |
| 70 – 98 | Life is full of good and bad, but we can be optimistic. | 18 (36%) |
| 98 – 112 | Everything is perfect! | - |
| Total | 50 | |
| LOT | Average Score Quality of life | Confidence interval | Dev. std | Min | Max | Q25 | Med. | Q75 | |
|---|---|---|---|---|---|---|---|---|---|
| LOT | Average Score Quality of life | -95% | -95% | Dev. std | Min | Max | Q25 | Med. | Q75 |
| Handball players | 61.34 | 56.55 | 66.13 | 16.85 | 30.00 | 88.00 | 47.00 | 63.50 | 75.00 |
| Test statistic: ANOVA, F(1, 49) =0.2833, p=0.5803 Levene Test of Homogeneity of Variances: F=1.6075, p=0.2023 | |||||||||
The distribution of cases according to the result of the quality of life assessment in the analysis shows that 24% (8 handball players) have a dysfunctional perception, while score values indicating the level of quality of life between 40 and 70 highlight a serious perception regarding life and the emphasis will be on the sense of duty to the detriment of well-being, we meet 40% of the representatives, and for score values between 70 - 98, where life must be treated detached because it is made up of good and bad but we can be optimistic, we meet a percentage of 36%.
The statistical indicators of the quality of life assessment score highlighted the absence of a significant difference (P = 0.5905) between the mean value of the quality of life score corresponding to the analyzed group (61.34 ± 16.85) with minimum values of 30 and maximum values of 88.
CONCLUSION
By its nature, handball is a sport of speed, with rapid changes of direction, with violent blocks, dives and aggressive fouls, in which overuse and the lack of prophylactic recovery programs are increasingly taking their toll. In an era of consumerism in which spectacle and sensationalism play a decisive role, limiting the occurrence of injuries becomes inevitable and the only reliable ally remains the responsibility with which the team around the athlete (doctor, coach, physiotherapist, psychologist) combines their approaches to form an athlete with an iron psyche and a physical condition that can brilliantly cope with the high-performance competition level and to limit as much as possible the occurrence of relapses where there was an injury in the past. The purpose of recovery programs is to strengthen the joints as much as possible, to develop strength, to increase the amplitude of movement because only with perfect physical training can the level of performance be maintained in the long term.
The values remaining after applying the questionnaire investigating the degree of limitation at the level of the studied limb confirm that 40% of the study participants face limitation in the shoulder joint, and thus their sports performance is affected, 48% complain of permanent pain in the injured joint, 66% of the participants experience episodes of insomnia and 52% report having a state of irritability in everyday life due to frustration regarding the limitation of daily activities but also due to the rest from sports life.
The analysis of all the data presented above shows that the degree of limitation regarding activities at the level of the injured shoulder is significant, the dysfunctions at the level of the injured shoulder lead to a low score regarding the quality of life of the athletes participating in the study and this fact contributes to a decrease in sports performance or to giving up on competitive sports. The quality of life of junior handball athletes with shoulder injuries depends largely on a complex and balanced recovery program, which addresses both physical, morphofunctional and psychological aspects. The evaluated athletes experienced states of denial, anger and even depression, which prevented the recovery process and at the same time a normalization of the score regarding the quality of life.